Rural vs Urban Health is not merely a matter of geography; it frames how communities experience prevention, access to care, and overall well-being. By comparing Rural health disparities with urban outcomes, we reveal patterns that highlight both barriers and opportunities for better care delivery. Urban health access in cities can be abundant, yet affordability and wait times still challenge many residents. Bridging rural-urban health gaps requires practical, scalable steps that can be implemented at local, regional, and national levels. This focus on Health equity rural urban signals a commitment to turning talk into actions that improve well-being for communities, whether in farms or neighborhoods.
Exploring the split in healthcare outcomes across geographic regions requires talking about geographic care gaps, remote care deserts, and the concentration of services in metropolitan networks. Rural-area wellness challenges often hinge on workforce shortages, longer travel times, and limited specialist access, while urban environments contend with high patient volumes and social determinants that complicate care delivery. By framing the topic in terms of geographic health disparities, access differentials, and systemic design, we can apply Latent Semantic Indexing principles to surface related concepts such as primary care integration, telemedicine readiness, and community-based outreach. The aim is to map connections between supply, demand, and social context so that strategies can be tailored to local realities. In short, the rural-urban health dialogue benefits from varied terminology that points to the same goal: equitable care for all, regardless of where people live.
Rural vs Urban Health: Mapping Disparities and Pathways to Equity
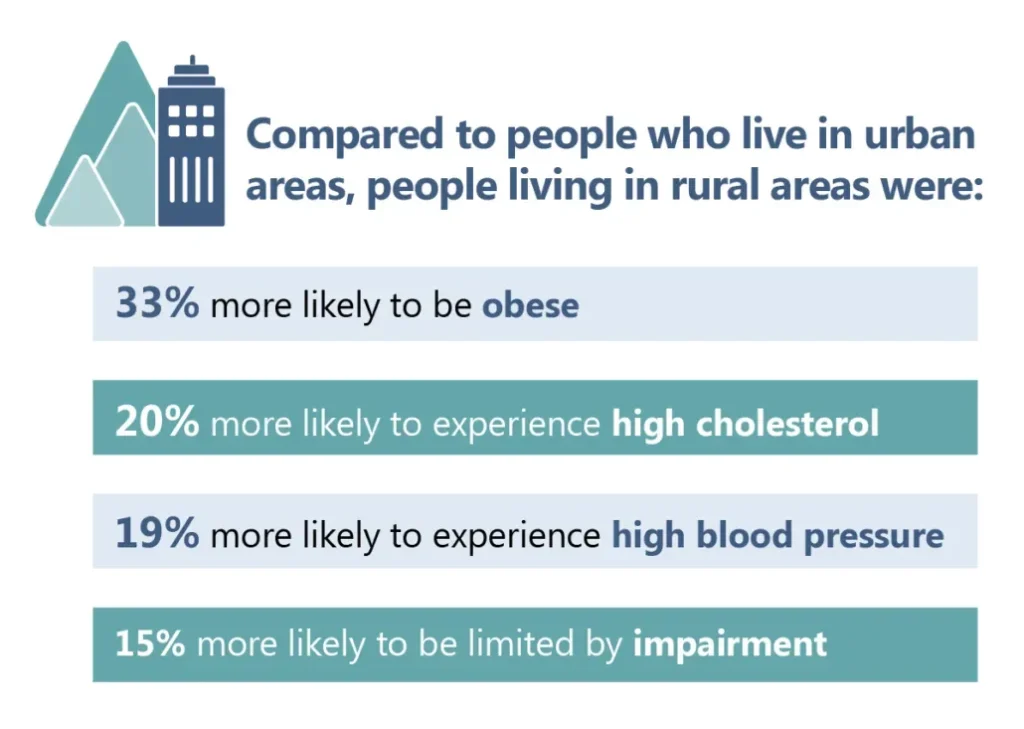
Rural vs Urban Health encompasses two distinct health ecosystems that shape access, outcomes, and daily life. Rural communities often contend with clinician shortages, longer travel times, and limited preventive services, which contribute to rural health disparities that manifest as higher burdens of chronic disease and delayed diagnoses. By contrast, urban settings typically offer greater provider density but grapple with overburdened clinics, long wait times, and social determinants that complicate access for low-income and marginalized residents. Together, these patterns form a complex map where geography and systems design drive equity—calling for practical, locally tailored reforms to improve health outcomes for all.
Understanding the landscape requires looking beyond distance to consider how care is organized, funded, and delivered. The contrast between Rural vs Urban Health highlights why targeted approaches are needed: expanding access, coordinating care, and addressing social determinants of health are essential to move toward true health equity rural urban. Recognizing these dynamics helps communities, providers, and policymakers design interventions that reduce wait times, improve preventive service uptake, and ensure that urban access and rural accessibility are treated as complementary parts of a unified health system.
Bridging rural-urban health gaps: Practical solutions for equitable care
A core theme in bridging rural-urban health gaps is expanding access through scalable, evidence-based strategies. Expanding telehealth and broadband access stands out as a powerful lever, especially when accompanied by reimbursement parity and user-friendly platforms. Mobile clinics and community-based care extend services into underserved areas, and CHWs or patient navigators can guide patients through appointments, transportation, and insurance enrollment. Together, these efforts tackle healthcare accessibility in rural areas while also connecting urban neighborhoods with local resources, demonstrated by practical steps like telemedicine for chronic disease management and preventive care.
Beyond access, strengthening care coordination and the workforce is essential. Integrating primary care with behavioral health and social services reduces fragmentation and supports health equity rural urban by aligning medical care with housing, transportation, and social supports. Investment in a resilient rural health workforce—through loan forgiveness, rural residency programs, and targeted funding for telehealth and interoperable EHRs—ensures sustainable capacity for both rural and urban populations. Coupled with data-driven measurement, partnerships, and community engagement, these actions create a scalable, observable shift toward bridging the gaps between rural health disparities and urban health access.
Frequently Asked Questions
In Rural vs Urban Health, what are rural health disparities and how does urban health access differ in practice?
Rural vs Urban Health shows that geography and how care is organized shape outcomes. Rural health disparities include clinician shortages, longer travel times, and lower preventive service use, while urban health access often features more providers but can suffer from overcrowding and wait times. Practical steps to bridge these gaps include expanding telehealth with reliable broadband, deploying mobile clinics, empowering community health workers, and improving care coordination—advancing health equity rural urban by connecting patients to timely services and social supports.
What strategies can advance health equity rural urban by improving Healthcare accessibility in rural areas and strengthening Urban health access through Bridging rural-urban health gaps?
Strategies combine place-based and system-wide actions. Expand telehealth, ensure reimbursement parity, and invest in broadband to improve Healthcare accessibility in rural areas; pair these with urban-focused efforts like integrated primary and behavioral health care and transportation supports to strengthen Urban health access. Data-driven planning, rural workforce development, and active community partnerships help Bridging rural-urban health gaps and advance Health equity rural urban for all residents.
| Aspect | Rural Health Characteristics | Urban Health Characteristics | Key Implications |
|---|---|---|---|
| Landscape & Comparison | Rural: Care organized with limited specialist access; longer travel for routine and specialized services; clinician shortages; higher burden of chronic disease management. | Urban: Greater provider concentration and facilities, but clinics can be overcrowded; longer wait times; social determinants still constrain access for low-income and marginalized groups. | Requires equity-focused, context-specific strategies and cross-setting collaboration to close gaps. |
| Geography & Access Barriers | Distances to clinics/hospitals can be a daily barrier; limited after-hours care; transportation gaps, especially for older adults and people with disabilities. | Distance is less of a barrier in many urban areas, but transportation costs, unsafe routes, schedules, and after-hours access remain challenges. | Address both physical access and scheduling across rural and urban contexts to reduce missed care and delays. |
| Workforce & Resources | Shortages of primary care physicians, nurses, and allied health staff; staffing strains; aging rural populations; limited preventive care capacity. | Urban clinics can be crowded with resource gaps in underserved pockets; providers may be concentrated but access can still be uneven. | Invest in workforce development, sustainable funding, and scalable clinic capacity to support preventive and chronic care in both settings. |
| Digital Divide & Care Coordination | Broadband limitations; slower speeds; variable digital literacy hamper telehealth and EHR interoperability in rural areas. | Data fragmentation and care coordination challenges across multiple urban providers and social services. | Expand interoperable technology, digital access, and shared care plans to connect providers and services across settings. |
| Social Determinants of Health | Poverty, housing instability, food insecurity, and limited health literacy; effects can be amplified by rural isolation. | Similar determinants in urban areas with concentrated risk factors and environmental stressors affecting access. | Address housing, transportation, nutrition, education, and health literacy to sustain improvements in both contexts. |
| Practical, Scalable Solutions | Expand telehealth and broadband; deploy mobile clinics; invest in community health workers; integrate primary and behavioral health; transportation support; data-driven planning. | Leverage similar solutions in urban areas with adaptations to dense settings and safety/after-hours considerations. | Scale feasible actions regionally; ensure policy support, funding, and evaluation to show real improvements. |
| Case Examples | Rural: Telehealth for endocrinology, mobile quarterly screenings, CHW-led education to improve screening and adherence. | Urban: Expanded after-hours telemedicine and transportation partnerships to reduce gaps for workers and caregivers. | Showcases how targeted, scalable actions can narrow gaps when funded, implemented, and evaluated. |
| Policy, Partnerships & Community Engagement | Incentives for rural practice; expanded telehealth reimbursement; broadband expansion; rural health funding mechanisms. | Urban partnerships; cross-sector collaboration; shared resources; emphasis on equity and housing/social supports. | Policy alignment with community needs and multi-stakeholder collaboration accelerates implementation. |
| Measuring What Matters | Access metrics (wait times, travel distance); preventive service uptake; chronic disease control; patient satisfaction; equity perceptions. | Comparable metrics for urban contexts, with emphasis on equity, patient experience, and social determinants. | Use real-time dashboards and transparent reporting to guide continuous improvement and accountability. |

